

Suprascapular Nerve Release
Arthroscopic Suprascapular Nerve Release and Treatment of Spinoglenoid Notch Cysts
Suprascapular neuropathy can lead to significant shoulder pain and functional limitation. It occurs when the suprascapular nerve is injured along is course either due to compression or traction. Cysts in the suprascapular or spinoglenoid notches can compress the nerve. Atrophy can occur of the rotator cuff muscles. Treatment is often dependent initial on if the disease is due to compression or traction. Surgical treatment if required often includes removal of the compressive lesion if one exists and release of the suprascapular ligament arthroscopically and possibly the spinoglenoid ligament at the levels of the suprascapular and spinoglenoid notches respectively.
Anatomy
The suprascapular nerve provides the motor and sensory function to the rotator cuff (supra and infraspinatus) as well as the joint capsule, acromioclavicular joint and subacromial bursa. The nerve originates from the brachial plexus and travels on the back side of the neck toward the scapula, through the suprascapular notch of the glenoid, on the floor of the supraspinatus fossa, around the spinoglenoid notch and then in the fossa of the infraspinatus. The neve gives off motor branches to the supraspinatus after it passes under the suprascapular ligament and several to the infraspinatus in the infraspinatus fossa.
Injury
The two locations of where the nerve is most commonly injured or entrapped is at the suprascapular and spinoglenoid notches. Traction or compression is often the reason for injury. Cysts resulting from labral tears of the posterosuperior labrum can compress the ligament at the suprascapular notch causing injury. Also , traction can result in injury from overhead use.
 Spinoglenoid notch cyst causing compression of the suprascapular nerve
Spinoglenoid notch cyst causing compression of the suprascapular nerve
History and physical examination
Patients often present with dull, aching shoulder pain in the back of the shoulder that is nonspecific. It is often not associated with use but can be exacerbated by activity that involves internal rotation and adduction. It can radiate into the neck or down the shoulder. Weakness if often more variable depending on what part of the nerve is involved or level of injury. If weakness is present it is often in external rotation or forward elevation. Young athletes commonly present with repetitive overhead activity that result in the problem as opposed to an isolated traumatic injury. On examination, other shoulder pathology and cervical spine pathology should be ruled out. There can be atrophy of the supraspinatus or infraspinatus fossa despite no injury to the tendon.
Imaging
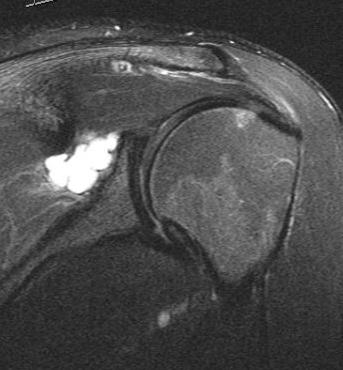
Xrays are typically normal in the setting of suprascapular neuropathy. MRI will often be normal in mild cases but can present with atrophy and neurogenic changes to the supraspinatus or infraspinatus muscle bellies or both. There is typically no injury to the rotator cuff tendon in isolated suprascapular neuropathy. In compression lesions, a cyst at the spinoglenoid or suprascapular notch is often present with an associated posterosuperior labral tear. EMG/NCV can demonstrate abnormalities including diminished amplitudes and increased conduction latency although patients can often have a diagnosis of suprascapular neuropathy with a normal EMG/NCV based off of history and physical examination. In cases of a normal EMG/NCV, a diagnostic local anesthetic injection will be performed under ultrasound. If pain relief occurs with a local injection, then a diagnosis of suprascapular neuropathy is confirmed.
 MRI image of a spinoglenoid notch cyst
MRI image of a spinoglenoid notch cyst
Treatment
In the setting of a compression lesion (cyst) with associated atrophy and EMG/NCV pathologic changes, early surgical intervention including cyst decompression and labral repair is recommended. The suprascapular ligament is often not released in these cases as traction at the notch is not the pathologic entity. In cases due to traction with EMG/NCV changes, a trial of conservative treatment including physical therapy, anti-inflammatories and a suprascapular nerve injection with anesthetic and cortisone can be performed to confirm and treat the disorder. Nonoperative treatment can be consider for 3 – 6 months with a repeat EMG/NCV. If there is progressive improvement in weakness and symptoms and the EMG is better, no surgical treatment is warranted. In patients with a diagnosis of suprascapular neuropathy without a space occupying lesion and without EMG/NCV changes, nonoperative treatment is reasonable for as long as the patient would like as there is no risk for long term damage but should be atleast attempted for 3 months.
In the setting of a compression lesion, then arthroscopic labral repair with cyst decompression should be performed. Arthroscopic treatment is outpatient. Patients are in a sling for 6 weeks working on range of motion exercises passively with a therapist and at home. At 6weeks, the patient is out of the sling using the arm for everyday activity with 10 lbs of lifting. At 3 months, strengthening is started with 30 lbs of lifting. At 4.5 months, 50 lbs of lifting is allowed and at 6 months the patient returns to all activities. Dr. Tashjian has described at technique for aspiration of the cyst during the surgical decompression and the published paper using this technique. (Robert Z Tashjian, Robert T Burks. Arthroscopic aspiration and labral repair for treatment of spinoglenoid notch cystsAm J Orthop (Belle Mead NJ). 2009 Feb;38(2):94-6.)
In the setting of a traction injury that has failed nonoperative treatment. The recommended treatment is an arthroscopic suprascapular ligament release. This is done in the outpatient setting. The arthroscope is placed into the subacromial space and the suprascapular ligament is observed as can be seen below.
 Suprascapular ligament is the white band of tissue running horizontally in the image
Suprascapular ligament is the white band of tissue running horizontally in the image
Once the suprascapular ligament is visualized, a switching stick is used to retract the nerve medially in the notch to protect it. A small basket punch is then brought in through a separate superior portal to release the ligament as can be seen in the image below.
 ligament has been released in this image compared to the prior image
ligament has been released in this image compared to the prior image
Once the ligament has been released, the nerve at the level of the suprascapular notch is completely free relieving any compression or tension on the nerve. A release nerve can be seen in the image below.
 The exposed suprascapular nerve which is the vertically oriented yellow
The exposed suprascapular nerve which is the vertically oriented yellow
If there is evidence of isolated spinoglenoid notch involvement, an isolated spinoglenoid ligament release can also be performed arthroscopically.
Postoperative from an arthroscopic suprascapular ligament release, patients are in a sling for comfort and allowed 10 lbs of lifting. Physical therapy is started at 2 weeks postoperative working on range of motion and strengthening. At 8 weeks postoperative, patients are allowed to return to all activities without restriction.



